iPhone Targeted Content

iPad Targeted Content
Android Targeted Content
Blackberry Targeted Content
Desktop and all none targeted content
iPhone Targeted Content
What Are You Adjusting? Hyper or Hypo?
June 03, 2010 by Dr Matthew D. Long
SHARE 
iPad Targeted Content
Android Targeted Content
What Are You Adjusting? Hyper or Hypo?
June 03, 2010 by Dr Matthew D. Long
SHARE
Blackberry Targeted Content
Desktop and all none targeted content
What Are You Adjusting? Hyper or Hypo?
June 03, 2010 by Dr Matthew D. Long
SHARE
To most chiropractors quality of spinal motion is a prerequisite for spinal health. We have an intrinsic understanding that a joint must move normally to be normal - or at least to stay that way. As such, our examinations are heavily geared towards assessing and quantifying the relative motion of each segment. We then give it a rating: 'normal', 'hypermobile' or 'hypomobile'.
Most of the time chiropractors tend to focus upon finding areas of limited motion - segments of greater stiffness that would benefit from an adjustment. Indeed, the majority of definitions of joint dysfunction suggest that reduced mobility is a cardinal sign, and that we should try to stay away from any hypermobile segment.
But is this really what's going on? Is it truly the stiffer joints that are the prime source of pain in most of our patients? And is it the stiffer joints that benefit the most from manipulation? Or could it actually be the hypermobile joints that should be the target of, and beneficiaries of, the neurological effects of an adjustment?
To look at this question we should briefly review the thrust (no pun intended) behind our last couple of Blog entries...
In Proprioception Part I (here) and Part II (here) we saw that patients suffering from chronic lower back pain seem to exhibit deficits of spinal sensation. They show a compromised ability to accurately position their torso and often demonstrate wasting of the segmental multifidus (a muscle that functions effectively as both a generator of muscular force and as proprioceptive apparatus). Such individuals also have greater postural sway and limited awareness of their trunk movements. The question is, does this lack of sensory acuity occur equally amongst complete regions of the spine (such as the lumbar or thoracic areas in their entirety), or is it actually the product of more limited segmental proprioceptive loss at one or two compromised levels?
You might recall from Proprioception Part II that there is clear evidence of cortical dysfunction amongst lower back pain patients. But other studies also suggest that instability and poor proprioception can also occur on a strictly segmental basis. And if this is the case, does diminished sensory feedback lead to joint hypermobility?
Could it be that many, if not most, of our lower back pain patients actually have hypermobile segments and not reduced joint motion?
A paper by Kulig et al (1) in 2007 compared MRI scans of both asymptomatic and symptomatic lumbar pain patients to see whether they differed in regards to segmental mobility. By using dynamic imaging via a vertically opened (double donut design) MRI system the researchers were able to quantify the amount of motion occurring at each lumbar level during both a PA mobilisation and during a prone self-extension manoeuvre.
They found that, "The symptomatic group had a larger percentage of subjects with evidence of single level segmental hypermobility than the asymptomatic group" and "This analysis suggests that a relatively high percentage of subjects in the symptomatic group demonstrated tendency towards hypermobility, especially at the L4-L5 and L5-S1 motion-segments."
Most of the time chiropractors tend to focus upon finding areas of limited motion - segments of greater stiffness that would benefit from an adjustment. Indeed, the majority of definitions of joint dysfunction suggest that reduced mobility is a cardinal sign, and that we should try to stay away from any hypermobile segment.
But is this really what's going on? Is it truly the stiffer joints that are the prime source of pain in most of our patients? And is it the stiffer joints that benefit the most from manipulation? Or could it actually be the hypermobile joints that should be the target of, and beneficiaries of, the neurological effects of an adjustment?
To look at this question we should briefly review the thrust (no pun intended) behind our last couple of Blog entries...
In Proprioception Part I (here) and Part II (here) we saw that patients suffering from chronic lower back pain seem to exhibit deficits of spinal sensation. They show a compromised ability to accurately position their torso and often demonstrate wasting of the segmental multifidus (a muscle that functions effectively as both a generator of muscular force and as proprioceptive apparatus). Such individuals also have greater postural sway and limited awareness of their trunk movements. The question is, does this lack of sensory acuity occur equally amongst complete regions of the spine (such as the lumbar or thoracic areas in their entirety), or is it actually the product of more limited segmental proprioceptive loss at one or two compromised levels?
You might recall from Proprioception Part II that there is clear evidence of cortical dysfunction amongst lower back pain patients. But other studies also suggest that instability and poor proprioception can also occur on a strictly segmental basis. And if this is the case, does diminished sensory feedback lead to joint hypermobility?
Could it be that many, if not most, of our lower back pain patients actually have hypermobile segments and not reduced joint motion?
A paper by Kulig et al (1) in 2007 compared MRI scans of both asymptomatic and symptomatic lumbar pain patients to see whether they differed in regards to segmental mobility. By using dynamic imaging via a vertically opened (double donut design) MRI system the researchers were able to quantify the amount of motion occurring at each lumbar level during both a PA mobilisation and during a prone self-extension manoeuvre.
They found that, "The symptomatic group had a larger percentage of subjects with evidence of single level segmental hypermobility than the asymptomatic group" and "This analysis suggests that a relatively high percentage of subjects in the symptomatic group demonstrated tendency towards hypermobility, especially at the L4-L5 and L5-S1 motion-segments."
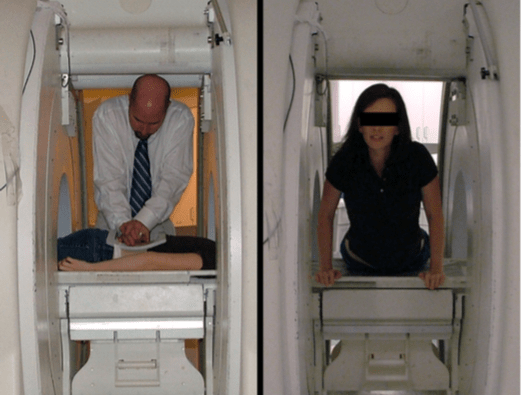
Figure 1. Subject and examiner positioned within the MRI system for (a) the segmental motion of the target lumbar segment during the posterior to anterior (PA) mobilization procedure and (b) the prone press-up PU maneuver. Each subject was situated such that the spine and torso were within the opening between the vertical magnets.
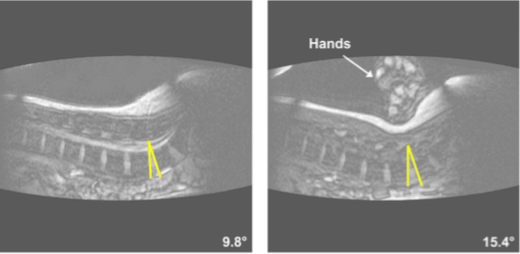
Figure 2. Measurements of intervertebral displacement resulting from the posterior to anterior (PA) mobilization. The intervertebral (segmental) angle was measured as the angle formed by lines defining the endplates of adjacent vertebrae. Segmental lumbar displacement was defined as the difference in the intervertebral angle between the resting position (left) and intervertebral angle from the end range image (right). The arrow in the image on the right identifies the hand of the examiner performing the PA mobilization.
This concept of hypermobility being a feature of spinal dysfunction was examined further by Lotz and Ulrich in the Journal of Bone and Joint Surgery (2). They characterised painful disc degeneration as possessing a triad of features, including; inflammation, annulus innervation and hypermobility. Indeed, hypermobility was seen as a prime motivator of the degenerative process, provoking further tissue breakdown and chemical sensitisation within the inner confines of the disc.
"The abnormal tissue stress associated with hypermobility may provoke disc cells to secrete proinflammatory factors that potentiate both inflammation and nociceptor sensitization. Certain types of mechanical stress can stimulate chondrocytes in ways similar to IL-1 and TNF-α... Tensile stretch also can increase the production of nitric oxide by anulus cells, resulting in a decrease in proteoglycan production."
So it seems that both degeneration and 'mechanical back pain' are often associated with hypermobility, not the stiffness and segmental hypomobility that is usually described. But why would chiropractors, physiotherapists and others consistently be looking for reduced joint motion as an indicator for manipulation?
Well, it appears that segmental instability (often in conjunction with multifidus wasting) prompts reflex contraction of the larger prime mover muscles of the trunk - such as the erector spinae. And it is this overlying muscle splinting that limits general torso movement and ultimately gives a sense of joint hypomobility to the examining clinician. In the end, it all comes back to proprioception...
If the brain is not receiving accurate sensory feedback about a spinal segment, and if it is not confident in its ability to regulate movement precisely, it will use muscular contraction to stiffen the joint.
But with multifidus wasting typically occurring after joint injury, the main segmental stabilisers are no longer available, so the brain has to use a different strategy to achieve its ends - the longer strap muscles.
Can we do anything to change this?
Well, it seems so. An adjustment to the spine does drive a burst of afferent activity through the proprioceptive pathways, largely via the muscle spindles.
Pickar and Kang (3), "suggest that spinal manipulation, when delivered manually with high velocity and low amplitude as a half-sinusoidal wave, engages an inherent signaling property belonging to the muscle spindle apparatus. We speculate that this provides a novel stimulus to the central nervous system because the ensuing spike trains from the population of muscle spindles are higher in frequency than that typically generated in groups Ia and II afferents from paraspinal muscles. Although voluntary motions of peripheral joints, for example, during locomotion, can stretch appendicular muscles sufficiently fast to elicit discharge frequencies over 200 Hz, we are not aware of data from axial tissues showing that voluntary trunk motion produces similar loading rates and elicits such high discharge frequencies. Nearly 3 decades ago, Korr proposed that spinal manipulation’s therapeutic effects may arise in part from the barrage of afferent impulses in muscle spindle afferents the central effects of which ultimately change motor circuits. Increasing evidence shows that short-lasting, high-frequency bursts from primary afferents can shape the function of spinal cord neurons."
Furthermore, such adjustments have been shown experimentally to increase the discharge frequency of primary afferent neurons from muscle spindles in the lumbar multifidus in an anaesthetised cat model (4) - something that might potentially help stimulate recruitment of these muscles and ultimately the stability of the spine. Indeed, a recent paper by Hair et al (5) showed that following manipulation of the lumbar spine patients "demonstrated increased lumbar multifidus thickness changes on the symptomatic side of pain that exceeded the minimal detectable change."
So could it be that many, or even most, of our symptomatic patients are suffering from joint hypermobility due to a proprioceptive deficit? And could it be that adjusting the spine is beneficial as it increases both the local sensory acuity of the segment and the recruitment of the multifidus muscle?
Perhaps it could...
Matthew D. Long
BSc (Syd) M.Chiro (Macq)
"The abnormal tissue stress associated with hypermobility may provoke disc cells to secrete proinflammatory factors that potentiate both inflammation and nociceptor sensitization. Certain types of mechanical stress can stimulate chondrocytes in ways similar to IL-1 and TNF-α... Tensile stretch also can increase the production of nitric oxide by anulus cells, resulting in a decrease in proteoglycan production."
So it seems that both degeneration and 'mechanical back pain' are often associated with hypermobility, not the stiffness and segmental hypomobility that is usually described. But why would chiropractors, physiotherapists and others consistently be looking for reduced joint motion as an indicator for manipulation?
Well, it appears that segmental instability (often in conjunction with multifidus wasting) prompts reflex contraction of the larger prime mover muscles of the trunk - such as the erector spinae. And it is this overlying muscle splinting that limits general torso movement and ultimately gives a sense of joint hypomobility to the examining clinician. In the end, it all comes back to proprioception...
If the brain is not receiving accurate sensory feedback about a spinal segment, and if it is not confident in its ability to regulate movement precisely, it will use muscular contraction to stiffen the joint.
But with multifidus wasting typically occurring after joint injury, the main segmental stabilisers are no longer available, so the brain has to use a different strategy to achieve its ends - the longer strap muscles.
Can we do anything to change this?
Well, it seems so. An adjustment to the spine does drive a burst of afferent activity through the proprioceptive pathways, largely via the muscle spindles.
Pickar and Kang (3), "suggest that spinal manipulation, when delivered manually with high velocity and low amplitude as a half-sinusoidal wave, engages an inherent signaling property belonging to the muscle spindle apparatus. We speculate that this provides a novel stimulus to the central nervous system because the ensuing spike trains from the population of muscle spindles are higher in frequency than that typically generated in groups Ia and II afferents from paraspinal muscles. Although voluntary motions of peripheral joints, for example, during locomotion, can stretch appendicular muscles sufficiently fast to elicit discharge frequencies over 200 Hz, we are not aware of data from axial tissues showing that voluntary trunk motion produces similar loading rates and elicits such high discharge frequencies. Nearly 3 decades ago, Korr proposed that spinal manipulation’s therapeutic effects may arise in part from the barrage of afferent impulses in muscle spindle afferents the central effects of which ultimately change motor circuits. Increasing evidence shows that short-lasting, high-frequency bursts from primary afferents can shape the function of spinal cord neurons."
Furthermore, such adjustments have been shown experimentally to increase the discharge frequency of primary afferent neurons from muscle spindles in the lumbar multifidus in an anaesthetised cat model (4) - something that might potentially help stimulate recruitment of these muscles and ultimately the stability of the spine. Indeed, a recent paper by Hair et al (5) showed that following manipulation of the lumbar spine patients "demonstrated increased lumbar multifidus thickness changes on the symptomatic side of pain that exceeded the minimal detectable change."
So could it be that many, or even most, of our symptomatic patients are suffering from joint hypermobility due to a proprioceptive deficit? And could it be that adjusting the spine is beneficial as it increases both the local sensory acuity of the segment and the recruitment of the multifidus muscle?
Perhaps it could...
Matthew D. Long
BSc (Syd) M.Chiro (Macq)
References:
1. Kulig K, Powers CM, Landel RF, Chen H, Fredericson M, Guillet M, Butts K. Segmental lumbar mobility in individuals with low back pain: in vivo assessment during manual and self-imposed motion using dynamic MRI. BMC Musculoskelet Disord. 2007 (8). http://www.biomedcentral.com/1471-2474/8/8
2. Lotz JC, Ulrich JA. Innervation, inflammation, and hypermobility may characterize pathologic disc degeneration: review of animal model data. Journal of bone and joint surgery American volume. 2006; 88.Suppl 2: pp. 76-82
3. Pickar JG, Kang YM. Paraspinal muscle spindle responses to the duration of a spinal manipulation under force control. J Manipulative Physiol Ther 2005; 29:22-31.
4. Pickar JG, Wheeler JD. Response of muscle proprioceptors to spinal manipulative-like loads in the anesthetized cat. J Manipulative Physiol Ther 2001; 24:2-11.
5. Hair LC, Raney NH, Gill NW, Teyhen DS. Quantification of Lumbar Multifidus Muscle Thickness Pre and Post Spinal Manipulation - An Ultrasound Imaging Cohort. Journal of Manual & Manipulative Therapy. 2009; 17 (3) pp. 1-2
1. Kulig K, Powers CM, Landel RF, Chen H, Fredericson M, Guillet M, Butts K. Segmental lumbar mobility in individuals with low back pain: in vivo assessment during manual and self-imposed motion using dynamic MRI. BMC Musculoskelet Disord. 2007 (8). http://www.biomedcentral.com/1471-2474/8/8
2. Lotz JC, Ulrich JA. Innervation, inflammation, and hypermobility may characterize pathologic disc degeneration: review of animal model data. Journal of bone and joint surgery American volume. 2006; 88.Suppl 2: pp. 76-82
3. Pickar JG, Kang YM. Paraspinal muscle spindle responses to the duration of a spinal manipulation under force control. J Manipulative Physiol Ther 2005; 29:22-31.
4. Pickar JG, Wheeler JD. Response of muscle proprioceptors to spinal manipulative-like loads in the anesthetized cat. J Manipulative Physiol Ther 2001; 24:2-11.
5. Hair LC, Raney NH, Gill NW, Teyhen DS. Quantification of Lumbar Multifidus Muscle Thickness Pre and Post Spinal Manipulation - An Ultrasound Imaging Cohort. Journal of Manual & Manipulative Therapy. 2009; 17 (3) pp. 1-2