iPhone Targeted Content

iPad Targeted Content
Android Targeted Content
Blackberry Targeted Content
Desktop and all none targeted content
iPhone Targeted Content
THE CLINICAL CLARITY BLOG
Migraine and stroke -
What's the connection?
JANUARY 19, 2019 by DR MATTHEW D. LONG
iPad Targeted Content
Android Targeted Content
THE CLINICAL CLARITY BLOG
Migraine and stroke -
What's the connection?
JANUARY 19, 2019 by DR MATTHEW D. LONG
Blackberry Targeted Content
Desktop and all none targeted content
THE CLINICAL CLARITY BLOG
JANUARY 19, 2019 by DR MATTHEW D. LONG
Migraine sufferers don't usually have an easy path in life. While their headache symptoms typically receive most of the attention, there is a potentially sinister side to the disorder that isn't often discussed. However, as chiropractors we should seek to understand this complex disease, as it is associated with another condition that we certainly wish to avoid - stroke.
Many clinicians do have a general appreciation for the neurological underpinnings of migraine. However, there is a tendency to focus upon the way in which a sufferer is susceptible to pain, particularly headaches. While this is clearly important, there is a significant body of evidence to show that the implications of migraine go far beyond any such pain symptoms (headaches or otherwise). Indeed, the disease was characterised by Burstein et al (1) thus,
Many clinicians do have a general appreciation for the neurological underpinnings of migraine. However, there is a tendency to focus upon the way in which a sufferer is susceptible to pain, particularly headaches. While this is clearly important, there is a significant body of evidence to show that the implications of migraine go far beyond any such pain symptoms (headaches or otherwise). Indeed, the disease was characterised by Burstein et al (1) thus,
"It is now viewed as a complex neurological disorder that affects multiple cortical, subcortical, and brainstem areas that regulate autonomic, affective, cognitive, and sensory functions. As such, it is evident that the migraine brain differs from the nonmigraine brain and that an effort to unravel the pathophysiology of migraine must expand beyond the simplistic view that there are 'migraine generator' areas."
One of the areas that has received the most attention in migraine research is the autonomic nervous system (ANS). There is mounting evidence that those affected exhibit numerous autonomic irregularities and are therefore unable to maintain homoeostasis when challenged. Indeed, some authors suggest that this 'dysautonomia' is the central pathophysiological feature of migraine, and that most of its symptom manifestations are an expression of this ANS lability. Gazerani and Cairns (2) write,
"Some, but not all evidence, suggests that migraine sufferers have a decreased sympathetic tone during headache free (interictal) periods compared with healthy individuals. Related to this, plasma norepinephrine concentrations are also approximately 50% lower than in healthy individuals, and the normal increase in plasma norepinephrine levels induced by the cold pressor test is blunted in migraine sufferers. Migraine sufferers also have responses that suggest alpha-adrenergic receptor super sensitivity, for example, they have an exaggerated pressor response (increased systolic and diastolic blood pressure) to the alpha adrenergic receptor agonist phenylephrine compared to health individuals. They also, as a group, tend to have a higher incidence of orthostatic hypotension than healthy controls."
And,
"In summary, current evidence from heart rate variability studies suggests that during the interictal phase there is an imbalance between the parasympathetic and sympathetic nervous systems. The bulk of the evidence does seem to support the concept that sympathetic tone is lowered during the interictal phase. During the headache phase, elevated systolic blood pressure (indicative of increased sympathetic tone) is found in some but not all studies."
THE CARDIOVASCULAR COMPLICATION
Clearly migraineurs are complex, and while the literature on ANS dysfunction in migraine is extensive and interesting, the point of this article is to focus attention upon a specific area of cardiovascular involvement that is not commonly discussed. In fact, there are two concerning attributes of the migraine patient that should give the average chiropractor reason to pause and think before applying treatment. These are:
1. Migraineurs have an increased risk of spontaneous stroke.
2. Migraine sufferers also present an increased risk for cerebrovascular complication to neck manipulation.
2. Migraine sufferers also present an increased risk for cerebrovascular complication to neck manipulation.
In general, those who experience migraine with an associated visual 'aura' are more likely to suffer an episode of ischaemic stroke than those without a history of headache (3). Furthermore, migraine-with-aura is independently associated with an increased risk of cardioembolic stroke when compared to the more common migraine-without-aura variant of the disease. A recent editorial in the journal Neurology by Fridman and Sposato (4) summarised it this way,
"Migraine with aura is an undisputed risk factor for ischemic stroke. Several mechanisms may mediate this risk, including genetic predisposition (e.g., NOTCH3, CACNA1A, SCN1A, ATP1A2); hypercoagulability (e.g., antiphospholipid antibodies, elevated von Willebrand factor and fibrinogen); hyperviscosity (polycythemia); increased platelet aggregability; hyperhomocysteinemia; elevated estrogens; paradoxical embolism from patent foramen ovale; and dissection of carotid, vertebral, or cerebral arteries."
Fridman and Sposato even asked the question 'Is migraine with aura an embolic TIA?' . This association between migraine-with-aura and cardioembolic stroke, and the parallel association between those with atrial fibrillation (AF) and subsequent stroke, prompted Sen et al (5) to investigate whether there was a specific link between migraine and AF. Might they be two sides of the same coin?
"Autonomic dysfunction has a significant role in influencing pathophysiology of both migraine and AF. Cardiac arrhythmia recordings have been shown to be present in ECGs of patients while experiencing migraine headaches as compared to migraine-free phases. This hypothesis is further supported by AF ablation procedures that have shown tendencies to reduce migraine symptoms and frequencies. This hypothesis then begs the question of whether migraine with aura development is attributable to cardioembolic stroke arising from the AF. The mediation analysis suggests that the migraine with visual aura stroke risk factor may be mediated via AF. It is possible that those with migraine with visual aura are at higher risk of AF due to autonomic dysfunction. The AF predisposes to left atrial thrombus formation and embolism into the brain resulting in cardioembolic stroke."
Now this does not suggest that all patients who suffer from migraine-with-aura are about to experience, or will ever experience, a significant cerebrovascular event. However, in Sen et al's study (5) the stroke incidence rate in the migraine-with-aura group (4.1/1,000 person-years) was approximately double that of the migraine-without-aura group (2.07/1,000 person-years).
The authors Tietjen et al (6) found that "selected vascular disease biomarkers are elevated in migraine, particularly in the subgroups most strongly linked to ischemic stroke risk – those with aura, and women." They also noted that it was the aura phenomenon itself, and not the actual headache symptoms, that strengthened the association with these disease markers. They further wrote,
The authors Tietjen et al (6) found that "selected vascular disease biomarkers are elevated in migraine, particularly in the subgroups most strongly linked to ischemic stroke risk – those with aura, and women." They also noted that it was the aura phenomenon itself, and not the actual headache symptoms, that strengthened the association with these disease markers. They further wrote,
"This study suggests that endothelial activation, as manifested by elevated biomarkers of hypercoagulability and inflammation, is associated with migraine, particularly in women. The correlation of biomarker levels with aura frequency and total number of aura-years suggests the possibility that aura is causally related to endothelial activation. If true, treatments that prevent aura, protect and repair the vasculature, or inhibit platelet aggregation and inflammation might prevent stroke in this at-risk subgroup of migraineurs. Whether elevated levels of these biomarkers are associated with subclinical MRI findings or with increased prevalence of patent foramen oval (PFO) in this population remains to be determined."
The need to recognise and manage any subclinical vascular deterioration becomes even more obvious when we see the relationship between migraine and white matter changes in the brain over time. Migraineurs, especially those with aura, are more likely than controls to exhibit white matter hyperintensities (WMHs) on MRI scans of their brain. These lesions are also associated with other vascular diseases such as hypertension, and are thought to reflect a reduction in blood perfusion (and therefore ischaemia). Fortunately the WMHs of migraine tend to be smaller than the 'confluent' changes that are typically seen with cerebrovascular disease and in cognitive decline. However, Eggers (7) suggested that the circumscribed lesions seen on a migraine sufferer's MRI are due to microemboli produced by platelet aggregation abnormalities. In turn, Xie and colleagues (8) found that "the degree and frequency of WMHs were positively correlated with unfavorable migraine prognosis." So it does appear that the structural changes occurring within the brains of our migraine patients may well predispose them to further suffering.
Yalcin and colleagues (9) studied the distribution of WMHs in patients with episodic migraine, and evaluated the distribution of lesions by hemisphere. Interestingly, they found that "deep/subcortical WMHs were dominantly accumulated in the cerebral hemisphere that was ipsilateral to the pain side." That is to say, those patients who primarily experienced migraines on one side of their head showed most of their white matter lesions on the same side.
Yalcin and colleagues (9) studied the distribution of WMHs in patients with episodic migraine, and evaluated the distribution of lesions by hemisphere. Interestingly, they found that "deep/subcortical WMHs were dominantly accumulated in the cerebral hemisphere that was ipsilateral to the pain side." That is to say, those patients who primarily experienced migraines on one side of their head showed most of their white matter lesions on the same side.
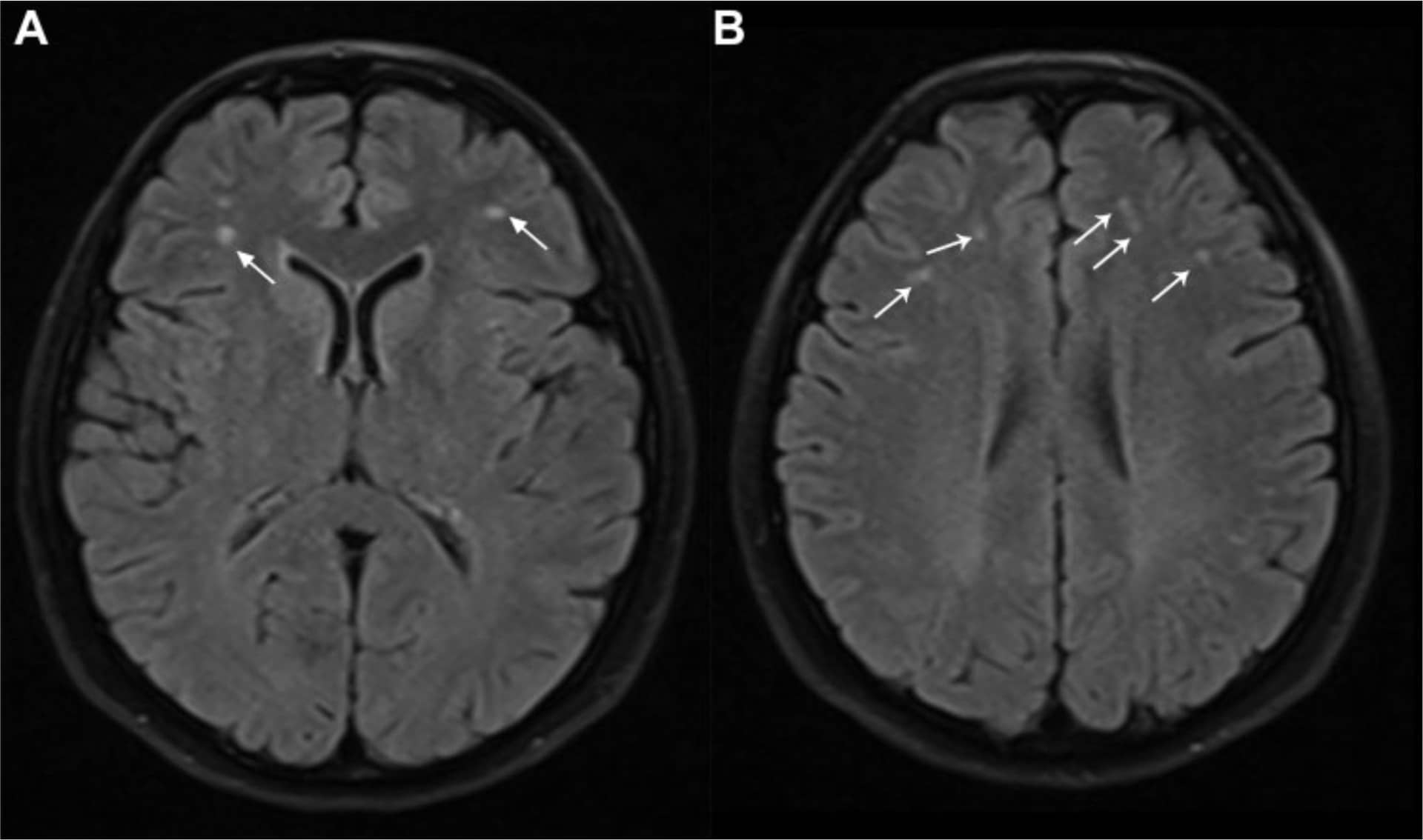
Axial FLAIR image (A) shows two subcortical white matter hyperintensities with a diameter of 3mm (arrows). More cranial images of the same patient (B) show additional deep and subcortical hyperintensities, which are smaller and have diameters ranging between 1 and 3 mm (arrows).
Image from: Yalcin, A., Ceylan, M., Bayraktutan, O. F., & Akkurt, A. (2018). Episodic Migraine and White Matter Hyperintensities: Association of Pain Lateralization. Pain Medicine (Malden, Mass), 19(10), 2051–2057. http://doi.org/10.1093/pm/pnx312
Image from: Yalcin, A., Ceylan, M., Bayraktutan, O. F., & Akkurt, A. (2018). Episodic Migraine and White Matter Hyperintensities: Association of Pain Lateralization. Pain Medicine (Malden, Mass), 19(10), 2051–2057. http://doi.org/10.1093/pm/pnx312
This seems important, as it draws a connection between the physiology of the migraine process itself, and the development of the lesions. Yalcin et al further state,
"There is an established connection between aura and deep white matter lesions. The mechanism is not clear, but it has been suggested that immediate hypoperfusion after a migraine attack is responsible. In contrast, imaging studies have demonstrated that hypoperfusion occurs in the aura phase, whereas hyperperfusion occurs in the pain phase. In our study, the patients tended to exhibit higher lesion counts in cerebral hemispheres that were ipsilateral to the pain side. We believe that this concordance is associated with disturbances in perfusion—both increases and decreases—in the cerebral parenchyma during the pain phase.
Considering mechanisms of both pain and WMH occurrence altogether with our study results, it is possible that pain and development of WMH in migraine might share a common mechanism, which should be the main target of treatment options. On this occasion, a clinician might be able to both treat pain and prevent lesion accumulation in the brain."
Considering mechanisms of both pain and WMH occurrence altogether with our study results, it is possible that pain and development of WMH in migraine might share a common mechanism, which should be the main target of treatment options. On this occasion, a clinician might be able to both treat pain and prevent lesion accumulation in the brain."
THE DISSECTION CONNECTION
Unfortunately the cardiovascular complications of migraine are not restricted to those individuals who fall into the 'visual aura' category. Indeed, those who experience the more common 'migraine-without-aura' variant pose an even greater concern to chiropractors, as they carry an increased risk of cervical artery dissection. Such dissections are of particular importance in young or middle-aged patients, and account for 10-20% of ischaemic strokes in those under 50 years of age (10). According to De Giuli and colleagues (11),
"In this large cohort study of patients with ischaemic stroke aged 18 to 45 years, we found a consistent association between migraine and spontaneous cervical artery dissection (CEAD). This association persisted after adjustment for traditional vascular risk factors, and it was apparent for the migraine subtype without aura more than for migraine with aura, for men more than for women, and for the younger rather than older age group."
But what is the mechanism? Why would a headache sufferer (albeit a highly complex one) have a greater tendency to spontaneous rupture of their arteries? Again, according to De Giuli et al,
"The mechanisms by which migraine might increase the individual propensity to CEAD remain unproven, but there are convincing arguments for common biological pathways underlying the 2 disorders. Among these, shared genetic susceptibility and endothelial dysfunction seem to be plausible."
From the genetic standpoint we know that cervical artery dissection is often associated with an underlying collagen disorder. Furthermore, the central role of an inherited connective tissue fragility seems even more likely when we note the higher prevalence of migraine amongst individuals with joint hypermobility syndromes (12,13). In a paper published in the journal Cephalalgia Bendik and colleagues (13) found,
"Our study indicates that the prevalence of migraine approaches 75% in female patients with joint hypermobility syndrome (JHS) and is 3 times greater in these patients than controls. The prevalence of tension-type headache was not increased, suggesting that the association between JHS and headache disorders is specific to migraine. The frequency and disability of migraine were also significantly increased in JHS patients. The increased risk of migraine in our JHS population supports the hypothesis of a common pathophysiology in these conditions."
Other connective tissue disorders, such as fibromuscular dysplasia, seem to have a predilection for the great vessels of the neck and head. And once again, there does seem to be an overlap between sufferers of this such disorders and migraineurs. In a paper entitled 'Fibromuscular Dysplasia: An Update for the Headache Clinician' (14), O'Connor and colleagues reported that a history of migraine was found "in 18% of those with carotid dissection and 23% of those with vertebral artery dissection."
So it does appear that some of our more flexible patients may be especially prone to weakening of their arterial walls. However, there are additional factors that increase the chance that our migraine-without-aura patients may suffer a cervical artery dissection. Mawet and colleagues (15) detailed a number of genetic associations between migraine and dissection risk. They also discussed the adverse effects of increased levels of matrix metalloproteinases (proteolytic enzymes involved in the homeostasis of the extracellular matrix), which may weaken the arterial wall and make it susceptible to spontaneous dissection during minimal or trivial trauma. These MMPs have been measured in higher concentrations in migraineurs and in those who have gone on to experience a cervical artery dissection.
In a similar vein (no pun intended), there has been significant research interest in the MTHFR gene polymorphism, which is involved in homocysteine metabolism, and a possible role in endothelial dysfunction. However, the most recent genome-wide association studies do not seem to support the initial flurry of enthusiasm for this line of research. As such, the jury is still out on the ultimate relevance of MTHFR.
I think that Giossi et al (16) summarises it best when they write,
So it does appear that some of our more flexible patients may be especially prone to weakening of their arterial walls. However, there are additional factors that increase the chance that our migraine-without-aura patients may suffer a cervical artery dissection. Mawet and colleagues (15) detailed a number of genetic associations between migraine and dissection risk. They also discussed the adverse effects of increased levels of matrix metalloproteinases (proteolytic enzymes involved in the homeostasis of the extracellular matrix), which may weaken the arterial wall and make it susceptible to spontaneous dissection during minimal or trivial trauma. These MMPs have been measured in higher concentrations in migraineurs and in those who have gone on to experience a cervical artery dissection.
In a similar vein (no pun intended), there has been significant research interest in the MTHFR gene polymorphism, which is involved in homocysteine metabolism, and a possible role in endothelial dysfunction. However, the most recent genome-wide association studies do not seem to support the initial flurry of enthusiasm for this line of research. As such, the jury is still out on the ultimate relevance of MTHFR.
I think that Giossi et al (16) summarises it best when they write,
"Overall, our findings are in line with the prevailing theory that spontaneous cervical artery dissection (sCeAD) represents a multifactorial disease and the end result of a synergistic interplay between an underlying constitutional arteriopathy and short-lasting environmental factors. These triggering factors, normally insufficient to induce arterial wall rupture alone, could transiently facilitate dissection in a fragile, previously asymptomatic, vessel wall."
As chiropractors it is vital that we understand and appreciate that our patients are highly individual, and present unique risk profiles when undergoing our treatment. We can certainly take comfort from recent research that supports the view that neck manipulation should not be seen as a singular cause of strokes (17,18,19). Rather, it appears that patients experiencing cervical artery dissection usually begin with symptoms of severe headache and neck pain, prompting them to seek out treatment, often from a chiropractor (20).
I have written on this topic previously in an article entitled 'The Stroke Perspective' here. Even so, we must remain vigilant when one of our migraine-suffering patients presents with symptoms that are just a bit different to normal, and when first deciding upon an appropriate treatment technique. We should not expect these individuals to look like someone who has obvious cardiovascular risk factors for stroke (such as obesity, hypertension or smoking). Indeed, the message from the literature is that there are a myriad of variables that might come into play, culminating in a final trivial inciting event.
I have written on this topic previously in an article entitled 'The Stroke Perspective' here. Even so, we must remain vigilant when one of our migraine-suffering patients presents with symptoms that are just a bit different to normal, and when first deciding upon an appropriate treatment technique. We should not expect these individuals to look like someone who has obvious cardiovascular risk factors for stroke (such as obesity, hypertension or smoking). Indeed, the message from the literature is that there are a myriad of variables that might come into play, culminating in a final trivial inciting event.
Something to think about...
Dr Matthew D. Long
BSc (Syd), M.Chiro (Macq)
Dr Matthew D. Long
BSc (Syd), M.Chiro (Macq)
References:
1. Burstein, R., Noseda, R., & Borsook, D. (2015). Migraine: multiple processes, complex pathophysiology. The Journal of Neuroscience, 35(17), 6619–6629. http://doi.org/10.1523/JNEUROSCI.0373-15.2015
2. Gazerani, P., & Cairns, B. E. (2018). Dysautonomia in the pathogenesis of migraine. Expert Review of Neurotherapeutics, 18(2), 153–165. http://doi.org/10.1080/14737175.2018.1414601
3. Androulakis, X. M., Kodumuri, N., Giamberardino, L. D., Rosamond, W. D., Gottesman, R. F., Yim, E., & Sen, S. (2016). Ischemic stroke subtypes and migraine with visual aura in the ARIC study. Neurology, 87(24), 2527–2532. http://doi.org/10.1212/WNL.0000000000003428
4. Fridman, S., & Sposato, L. A. (2018). Migraine with visual aura, incident AF, and stroke risk: Is migraine with aura an embolic TIA? Neurology. http://doi.org/10.1212/WNL.0000000000006637
5. Sen, S., Androulakis, X. M., Duda, V., Alonso, A., Chen, L. Y., Soliman, E. Z., et al. (2018). Migraine with visual aura is a risk factor for incident atrial fibrillation: A cohort study. Neurology, 91(24), e2202–e2210. http://doi.org/10.1212/WNL.0000000000006650
6. Tietjen, G. E., Khubchandani, J., Herial, N., Palm-Meinders, I. H., Koppen, H., Terwindt, G. M., et al. (2018). Migraine and vascular disease biomarkers: A population-based case-control study. Cephalalgia, 38(3), 511–518. http://doi.org/10.1177/0333102417698936
7. Eggers AE. Migraine white matter hyperintensities and cerebral microinfarcts are silent cryptogenic strokes and relate to dementia. Med Hypotheses. 2017;102:1–3.
8. Xie, H., Zhang, Q., Huo, K., Liu, R., Jian, Z.-J., Bian, Y.-T., et al. (2018). Association of white matter hyperintensities with migraine features and prognosis. BMC Neurology, 18(1), 629–10. http://doi.org/10.1186/s12883-018-1096-2
9. Yalcin, A., Ceylan, M., Bayraktutan, O. F., & Akkurt, A. (2018). Episodic Migraine and White Matter Hyperintensities: Association of Pain Lateralization. Pain Medicine (Malden, Mass), 19(10), 2051–2057. http://doi.org/10.1093/pm/pnx312
10. Thomas, L. C., Makaroff, A. P., Oldmeadow, C., Attia, J. R., & Levi, C. R. (2017). Seasonal variation in cervical artery dissection in the Hunter New England region, New South Wales, Australia: A retrospective cohort study. Musculoskeletal Science & Practice, 27, 106–111. http://doi.org/10.1016/j.math.2016.10.007
11. De Giuli, V., Grassi, M., Lodigiani, C., Patella, R., Zedde, M., Gandolfo, C., et al. (2017). Association Between Migraine and Cervical Artery Dissection: The Italian Project on Stroke in Young Adults. JAMA Neurology, 74(5), 512–518. http://doi.org/10.1001/jamaneurol.2016.5704
12. Puledda, F., Viganò, A., Celletti, C., Petolicchio, B., Toscano, M., Vicenzini, E., et al. (2015). A study of migraine characteristics in joint hypermobility syndrome a.k.a. Ehlers-Danlos syndrome, hypermobility type. Neurological Sciences, 36(8), 1417–1424. http://doi.org/10.1007/s10072-015-2173-6
13. Bendik, E. M., Tinkle, B. T., Al-shuik, E., Levin, L., Martin, A., Thaler, R., et al. (2011). Joint hypermobility syndrome: A common clinical disorder associated with migraine in women. Cephalalgia, 31(5), 603–613. http://doi.org/10.1177/0333102410392606
14. O'Connor, S. C., Poria, N., & Gornik, H. L. (2015). Fibromuscular dysplasia: an update for the headache clinician. Headache, 55(5), 748–755. http://doi.org/10.1111/head.12560
15. Mawet, J., Debette, S., Bousser, M.-G., & Ducros, A. (2016). The Link Between Migraine, Reversible Cerebral Vasoconstriction Syndrome and Cervical Artery Dissection. Headache, 56(4), 645–656. http://doi.org/10.1111/head.12798
16. Giossi, A., Ritelli, M., Costa, P., Morotti, A., Poli, L., Del Zotto, E., et al. (2014). Connective tissue anomalies in patients with spontaneous cervical artery dissection. Neurology, 83(22), 2032–2037. http://doi.org/10.1212/WNL.0000000000001030
17. Cassidy JD, Boyle E, Cote P, He Y, Hogg-Johnson S, Silver FL, et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study. Spine 2008;33(suppl 4):S176-83.
18. Tuchin, P. (2013). Chiropractic and stroke: association or causation? International Journal of Clinical Practice, 67(9), 825–833. doi:10.1111/ijcp.12171
19. Church, E. W., Sieg, E. P., Zalatimo, O., Hussain, N. S., Glantz, M., & Harbaugh, R. E. (2016). Systematic Review and Meta-analysis of Chiropractic Care and Cervical Artery Dissection: No Evidence for Causation. Cureus, 8(2), e498. http://doi.org/10.7759/cureus.498
20. Kosloff, T. M., Elton, D., Tao, J., & Bannister, W. M. (2015). Chiropractic care and the risk of vertebrobasilar stroke: results of a case-control study in U.S. commercial and Medicare Advantage populations. Chiropractic & Manual Therapies, 23, 19. http://doi.org/10.1186/s12998-015-0063-x
1. Burstein, R., Noseda, R., & Borsook, D. (2015). Migraine: multiple processes, complex pathophysiology. The Journal of Neuroscience, 35(17), 6619–6629. http://doi.org/10.1523/JNEUROSCI.0373-15.2015
2. Gazerani, P., & Cairns, B. E. (2018). Dysautonomia in the pathogenesis of migraine. Expert Review of Neurotherapeutics, 18(2), 153–165. http://doi.org/10.1080/14737175.2018.1414601
3. Androulakis, X. M., Kodumuri, N., Giamberardino, L. D., Rosamond, W. D., Gottesman, R. F., Yim, E., & Sen, S. (2016). Ischemic stroke subtypes and migraine with visual aura in the ARIC study. Neurology, 87(24), 2527–2532. http://doi.org/10.1212/WNL.0000000000003428
4. Fridman, S., & Sposato, L. A. (2018). Migraine with visual aura, incident AF, and stroke risk: Is migraine with aura an embolic TIA? Neurology. http://doi.org/10.1212/WNL.0000000000006637
5. Sen, S., Androulakis, X. M., Duda, V., Alonso, A., Chen, L. Y., Soliman, E. Z., et al. (2018). Migraine with visual aura is a risk factor for incident atrial fibrillation: A cohort study. Neurology, 91(24), e2202–e2210. http://doi.org/10.1212/WNL.0000000000006650
6. Tietjen, G. E., Khubchandani, J., Herial, N., Palm-Meinders, I. H., Koppen, H., Terwindt, G. M., et al. (2018). Migraine and vascular disease biomarkers: A population-based case-control study. Cephalalgia, 38(3), 511–518. http://doi.org/10.1177/0333102417698936
7. Eggers AE. Migraine white matter hyperintensities and cerebral microinfarcts are silent cryptogenic strokes and relate to dementia. Med Hypotheses. 2017;102:1–3.
8. Xie, H., Zhang, Q., Huo, K., Liu, R., Jian, Z.-J., Bian, Y.-T., et al. (2018). Association of white matter hyperintensities with migraine features and prognosis. BMC Neurology, 18(1), 629–10. http://doi.org/10.1186/s12883-018-1096-2
9. Yalcin, A., Ceylan, M., Bayraktutan, O. F., & Akkurt, A. (2018). Episodic Migraine and White Matter Hyperintensities: Association of Pain Lateralization. Pain Medicine (Malden, Mass), 19(10), 2051–2057. http://doi.org/10.1093/pm/pnx312
10. Thomas, L. C., Makaroff, A. P., Oldmeadow, C., Attia, J. R., & Levi, C. R. (2017). Seasonal variation in cervical artery dissection in the Hunter New England region, New South Wales, Australia: A retrospective cohort study. Musculoskeletal Science & Practice, 27, 106–111. http://doi.org/10.1016/j.math.2016.10.007
11. De Giuli, V., Grassi, M., Lodigiani, C., Patella, R., Zedde, M., Gandolfo, C., et al. (2017). Association Between Migraine and Cervical Artery Dissection: The Italian Project on Stroke in Young Adults. JAMA Neurology, 74(5), 512–518. http://doi.org/10.1001/jamaneurol.2016.5704
12. Puledda, F., Viganò, A., Celletti, C., Petolicchio, B., Toscano, M., Vicenzini, E., et al. (2015). A study of migraine characteristics in joint hypermobility syndrome a.k.a. Ehlers-Danlos syndrome, hypermobility type. Neurological Sciences, 36(8), 1417–1424. http://doi.org/10.1007/s10072-015-2173-6
13. Bendik, E. M., Tinkle, B. T., Al-shuik, E., Levin, L., Martin, A., Thaler, R., et al. (2011). Joint hypermobility syndrome: A common clinical disorder associated with migraine in women. Cephalalgia, 31(5), 603–613. http://doi.org/10.1177/0333102410392606
14. O'Connor, S. C., Poria, N., & Gornik, H. L. (2015). Fibromuscular dysplasia: an update for the headache clinician. Headache, 55(5), 748–755. http://doi.org/10.1111/head.12560
15. Mawet, J., Debette, S., Bousser, M.-G., & Ducros, A. (2016). The Link Between Migraine, Reversible Cerebral Vasoconstriction Syndrome and Cervical Artery Dissection. Headache, 56(4), 645–656. http://doi.org/10.1111/head.12798
16. Giossi, A., Ritelli, M., Costa, P., Morotti, A., Poli, L., Del Zotto, E., et al. (2014). Connective tissue anomalies in patients with spontaneous cervical artery dissection. Neurology, 83(22), 2032–2037. http://doi.org/10.1212/WNL.0000000000001030
17. Cassidy JD, Boyle E, Cote P, He Y, Hogg-Johnson S, Silver FL, et al. Risk of vertebrobasilar stroke and chiropractic care: results of a population-based case-control and case-crossover study. Spine 2008;33(suppl 4):S176-83.
18. Tuchin, P. (2013). Chiropractic and stroke: association or causation? International Journal of Clinical Practice, 67(9), 825–833. doi:10.1111/ijcp.12171
19. Church, E. W., Sieg, E. P., Zalatimo, O., Hussain, N. S., Glantz, M., & Harbaugh, R. E. (2016). Systematic Review and Meta-analysis of Chiropractic Care and Cervical Artery Dissection: No Evidence for Causation. Cureus, 8(2), e498. http://doi.org/10.7759/cureus.498
20. Kosloff, T. M., Elton, D., Tao, J., & Bannister, W. M. (2015). Chiropractic care and the risk of vertebrobasilar stroke: results of a case-control study in U.S. commercial and Medicare Advantage populations. Chiropractic & Manual Therapies, 23, 19. http://doi.org/10.1186/s12998-015-0063-x